How Will COVID-19 Unfold in 2020’s Second Half?

Editor’s Note: The following article is part of an ongoing series offering our strategic advice and expertise on what healthcare industry stakeholders should do immediately in response to the rapidly evolving novel coronavirus (COVID-19) pandemic.
The first half of 2020 was marked by the emergence of COVID-19 and its rapid global spread. Countries navigated their way through initial suppression and in recent weeks, tentative reopening. Early questions revolved around potential scenarios – three months, six months, and beyond. As we described in May (The Long Haul), we have now entered the long haul of suppression, with the virus becoming endemic, flaring periodically in various geographies. The virus could be eradicated with the invention and global distribution of an effective vaccine, a cure, or a therapeutic that drastically reduces the burden of the disease; eradication of the virus may also be aided by rising herd immunity if natural infection confers protection for significant enough periods.
Questions now revolve around a longer time frame – what does the rest of the year look like? How do we return to work and school and manage economic activity while co-existing with the virus? How much of our previous, normal lives and economy can we reclaim without new waves of infection that threaten to overwhelm our health system? Below, we lay out our perspective on these key questions.
Many countries across the world and all US states have made steps towards reopening; many have well over a month of reopening behind them while others are just now entering their first and second phases of reopening. As per Exhibit 1 below, the United States in particular is seeing increasing new case counts and hospitalizations by at least 10 percent in 39 states, largely clustered in the South and West of the country.
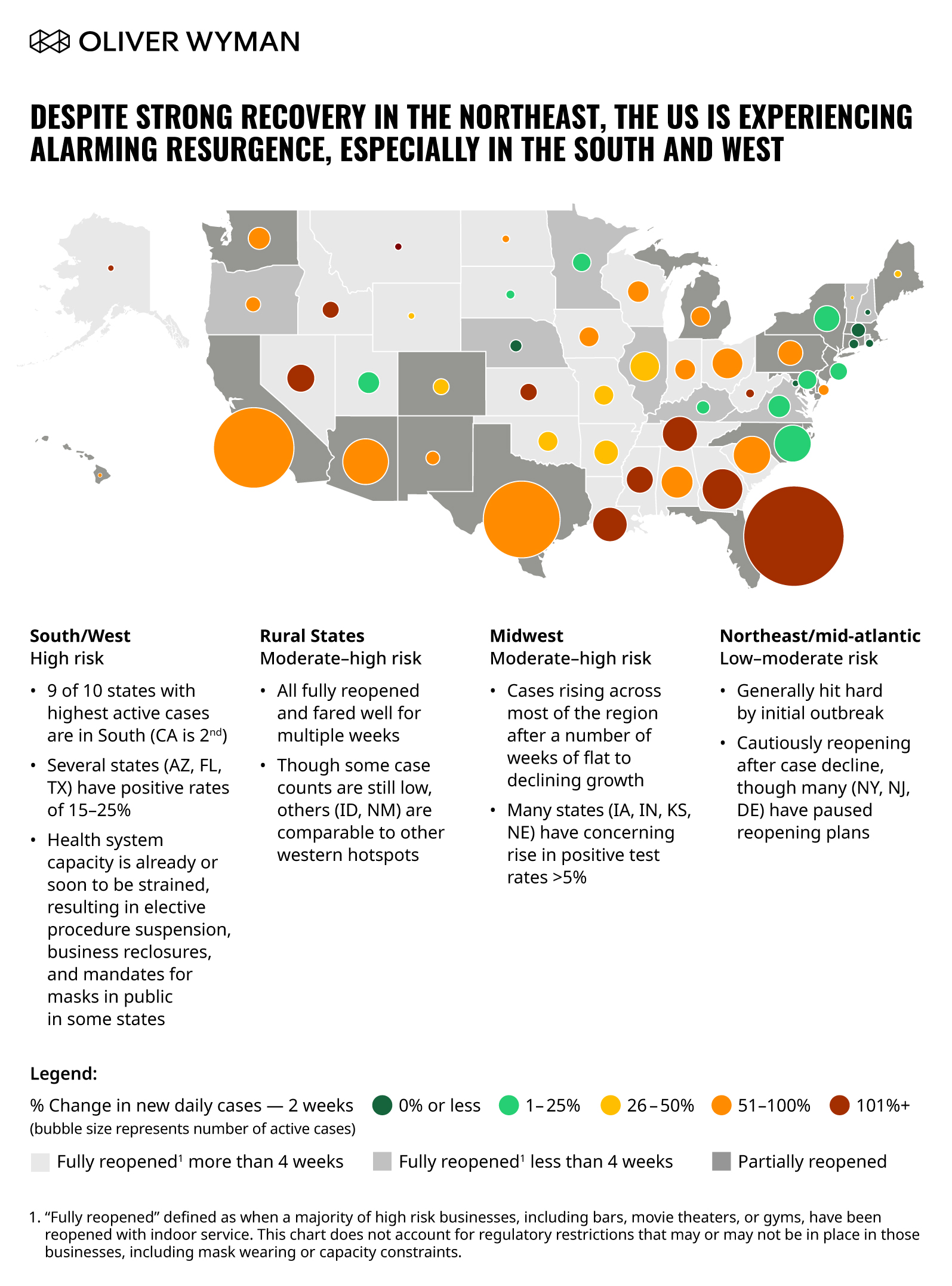
Of concern are states with high levels of total active infections (including estimated undetected cases) per million (such as Arizona, South Carolina, Arkansas, Texas, Florida, Mississippi, and Alabama) and an instantaneous reproduction rate R(t) significantly greater than 1, leading to exponential growth of active cases and new cases.
As we have mentioned repeatedly, some resurgence of the virus is expected, but why have these states seen such alarming growth? There are multiple reasons, but here are the main ones:
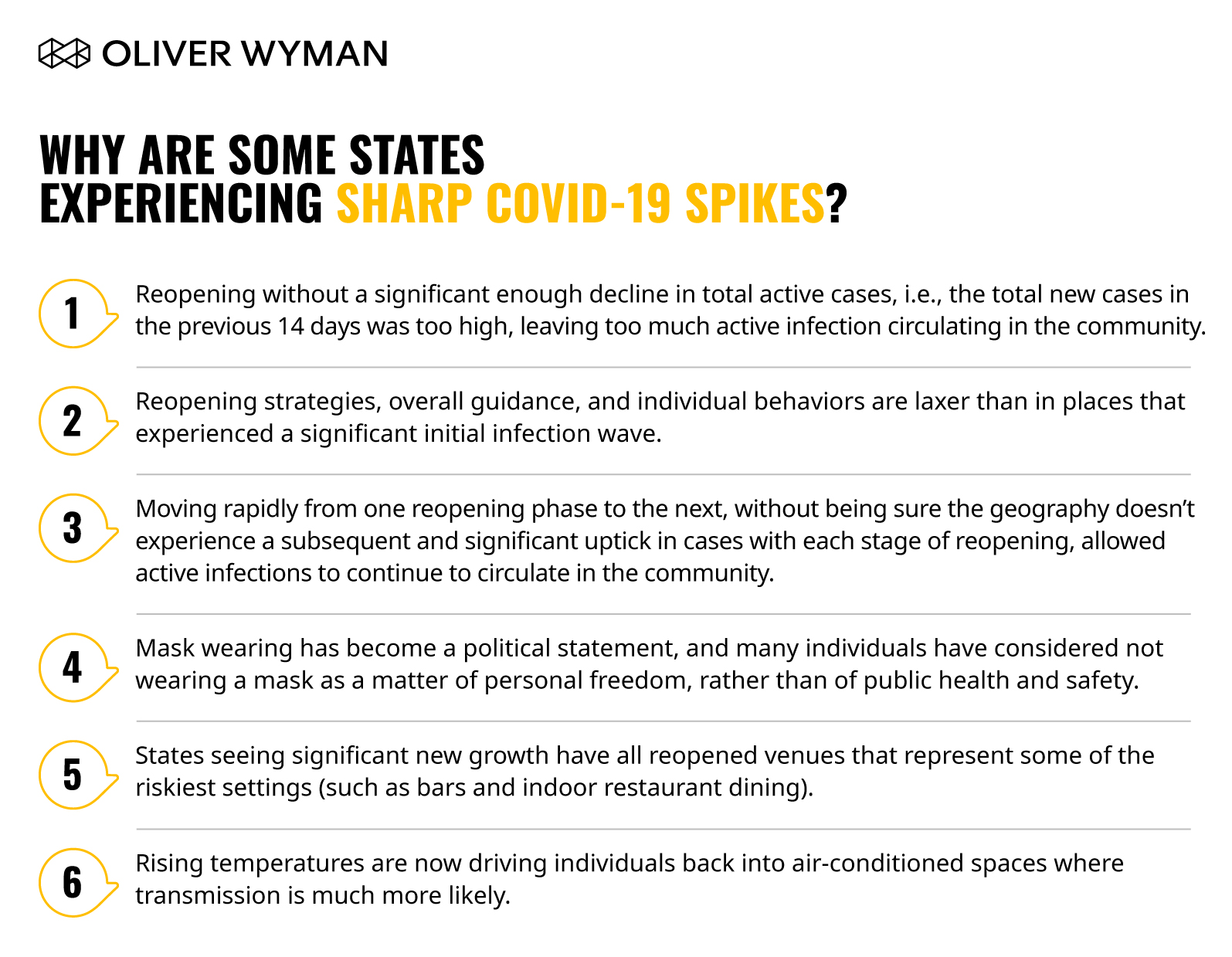
First, reopening without a significant enough decline in total active infections, simply put, meant the total of new cases from the past 14 days left too many active cases circulating in the community. To use an analogy with forest fires, the number of active cases represents the current size of the forest fire. Achieving R(t) below 1 gives us an indication that the fire is beginning to shrink but it is clearly also important to understand how big the fire is before deciding whether it is an appropriate time to reduce measures to contain it. A large but shrinking fire is as much of a concern as a small but growing fire.
Second, states (and individuals therein) spared early may not have had a full appreciation for the impact that nearly exponential spread of the virus could have in their geography (for example, overwhelmed hospital systems and the worsening of outcomes for unrelated diseases and conditions). As a result, reopening strategy, overall guidance, and individual behavior are more lax than in places that experienced a significant wave of infections initially.
Third, reopening too rapidly between phases without time to measure the impact of each phase was detrimental. While the number of undetected cases (for example, asymptomatic cases) is not directly observable, it should be factored into any decision. Otherwise, we would underestimate the total size of the problem. Our best estimate for total cases is currently six times, and could be as high as 10 times, the number of confirmed cases in the US. This translates to between five and eight percent of the total population. For Mexico, where testing per population is very low, our best estimate is undetected cases are 38 times confirmed cases.
Fourth, consider lax guidance on/lack of compliance with behaviors that prevent transmission. Driven by a combination of political stances, personal beliefs, and quarantine fatigue, perhaps exacerbated by weeks of mass public protests, we have seen significant variation between states concerning mask wearing and social distancing. We know from multiple research studies these behaviors work to reduce transmission. (For example, a Lancet study suggested just one meter of physical distance could reduce the chance of infection by up to ten percentage points). We see a strong correlation between behavior and case growth. Sixteen states recommend, but do not require, their residents wear masks in public. In those states, new coronavirus cases have risen by 92 percent over the last two weeks. In the 15 states that have mandated wearing masks in public for at least a month, new cases have risen by only 17 percent over the last two weeks. Mask wearing has (unfortunately) become a political statement and many individuals have considered not wearing a mask a matter of personal freedom, rather than of public health and safety. In addition to the actual protection they provide, masks serve as a reinforcement of on-going vigilance – they signal, “we know this isn’t over and we are continuing to keep each other safe.”
Fifth, rapid re-opening of some of the riskiest settings (such as bars and indoor restaurant dining) exacerbated transmission. States seeing significant new growth have all reopened these venues to some degree. Not only are these venues riskier due to sustained, proximal interaction between individuals in a setting with recirculating air, but the atmosphere could contribute to increasingly risky behavior (for example, noisy environments drive individuals to shout and sit or stand in close proximity to each other, and consuming alcohol lowers inhibitions around maintaining distance). While there is substantial variation in hygiene, distancing, and capacity requirements by region, in the 13 states (including DC) that had not reopened indoor bars by mid-June, new cases have fallen by three percent over the past two weeks. In the 38 states that had reopened indoor bars, cases had risen by 98 percent over the past two weeks.
Lastly, rising temperatures are driving individuals back into air-conditioned spaces such as gyms, restaurants, and bars where transmission is much more likely, since rapidly recirculating air gives momentum for the virus to travel distances within closed spaces.
This coronavirus is novel, meaning it’s new in humans and as of yet we have no ‘herd immunity’ to it. Without mitigation efforts, it is very contagious. We know the virus spreads efficiently through the air and is transmitted through speaking (especially by coughs and sneezes within three to six feet), and actions like singing and shouting at greater distances. Further complicating matters, a large number of infected people may show no symptoms but can still transmit the virus to others. Therefore, this is not just about asking the obviously symptomatic to self-isolate. It’s about asking everyone to take measures to protect one another. Here are several considerations:
First, certain situations place people at a greater infection risk. These include tight living quarters (such as group homes, nursing homes, homeless shelters, and crew quarters on ships), places where people are in enclosed spaces for long periods (such as bars, restaurants, churches, and movie theaters), retail settings where staff have continuous and close contact with the public, and any air-conditioned crowded spaces with rapidly recirculating air.
Second, certain groups are at higher risk of developing severe infections resulting in hospitalization, and death. For a variety of reasons, these include people over 60 years old, people with underlying lung, heart, cancer, or diabetes diagnoses, as well as people of lower socioeconomic status.
Third, infecting others can be reduced by (all) people wearing masks in public, practicing social distancing, frequent handwashing, and asking those who are infected (and their close contacts) to quarantine.
Fourth, individuals with infections respond by developing antibodies thought to protect them from reinfection periods, though we currently don’t know for how long. Individuals with asymptomatic infections appear to develop lower levels (and in some, no levels) of antibodies. Whether these people are protected is unknown.
Fifth, certain COVID-19 positive patients suffer long-lasting damages and illnesses even after they test negative and have “recovered” from the virus.
Lastly, fear of the virus, the isolation and loneliness of shutdowns, the financial worries, and disruption from potential subsequent lockdowns to suppress a rapid resurgence lead to anxiety and mental health concerns.
From a public health perspective, the main goals of suppression measures have always been to protect the highest-risk people and to manage the number of infections below hospital system capacity to allow clinicians to care for COVID-19 patients AND the patients with everyday illnesses in their communities (such as heart attacks, strokes, appendicitis, and cancer). Doing this can protect economic health by giving employees and consumers confidence in the geography’s ability to contain the virus.
So What Do We Do Now?
In short, get R(t) of total cases under control in places where it has increased to the extent that hospital capacity is threatened or has been exceeded. Elsewhere, keep as much of the economy open as possible – particularly in temperate months where outdoor activity is easily managed (in the US, for example, this includes Summer and early Fall in the Northeast and Midwest regions, or Fall and Winter in the South).
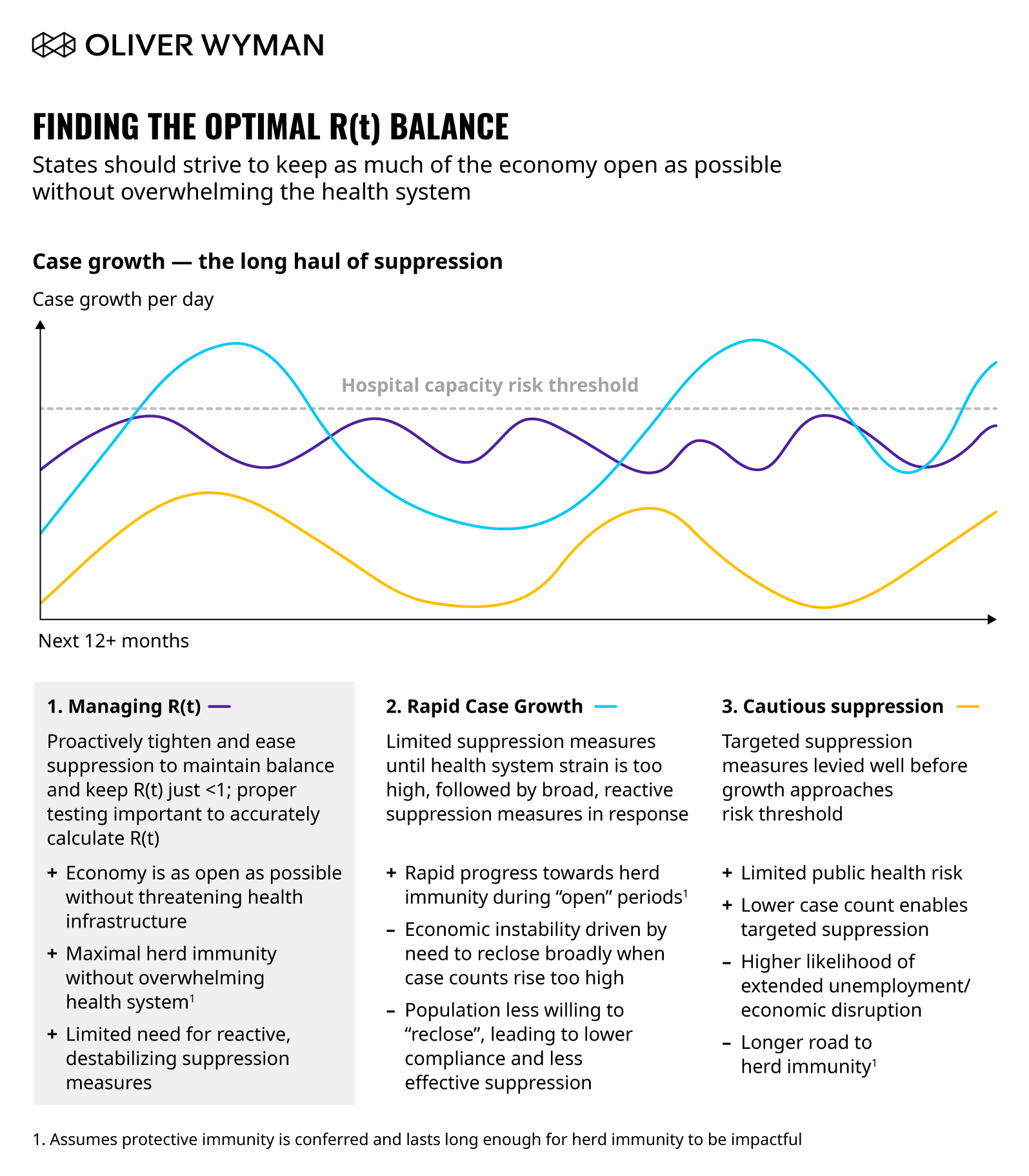
As per the above exhibit, aside from revitalizing the economy, a potential benefit of this approach is the accelerated progress towards achieving herd immunity, if infection confers protective immunity for a significant enough time (ideally, at least a year). Here are five suggestions on how to do this:
1. Understand hospital capacity thresholds – particularly intensive care unit (ICU) capacity in each geography – and closely monitor them to understand how R(t) is changing, for how many days you can afford to run at that R(t) before breaching hospital capacity, and what options will slow down R(t).
The better we understand this and the more time we have to act, the better we can make smaller, timely adjustments and prevent the need for blunt lockdown measures. For example, regions across New York must have at least 30 percent of ICU and hospital beds open to move forward with reopening, and the local government has indicated it will reverse course in regions with substandard figures.
In states with significant new growth, we are already facing new disruption risks. On June 25, Texas Governor, Greg Abbott, issued an executive order suspending elective procedures in four Texas counties given the rapid rise of cases in Dallas. Despite “abundant” capacity on June 22nd, now current projections show Dallas Fort-Worth (DFW) reaching full capacity as soon as mid-July, though surge capacity is ready to be deployed. As cases rise, we expect more pauses on elective procedures to follow – leading to significant financial ramifications to health systems already damaged by revenue loss in the last few months. In early July, Abbott mandated that Texans living in counties with more than 20 coronavirus cases wear a face covering in public.
2. Decouple mobility from transmission through the right behaviors.
During the pandemic’s early stages when we were sheltering in mass scale, mobility rates and the transmission rate of the virus were tightly correlated. As we reopen, however, we are learning about the impact of allowing certain activities to resume, and that mobility and the transmission rates are not always tightly correlated. We've also learned from the examples set by other countries who experienced outbreaks before the US. Some countries (like Germany and Norway) have seen their population’s mobility increase without significant increases in the spread of the virus. We believe this is driven in part by learned behavior – wearing masks, washing hands, keeping socially distant, and conducting continuous screenings with selective quarantines for those who test positive. Countries and states that have made this a part of their culture (often in response to experiencing a “tsunami” first wave, or experience with a prior pandemic), are seeing greater reopening success. In the US, this culture must be made more consistent across states and reinforced by the government and private sector. Employers are well-positioned to educate and influence their employees to drive the right kind of behavior (such as mask wearing, social distancing, and self-reporting symptoms without fear of repercussions). This will require consistent and repeated messaging, the right forms of support (including mental health and wellbeing), and appropriate policies (such as no loss of pay if an individual has symptoms and needs to stay home).
3. Shift towards safe(r) interactions.
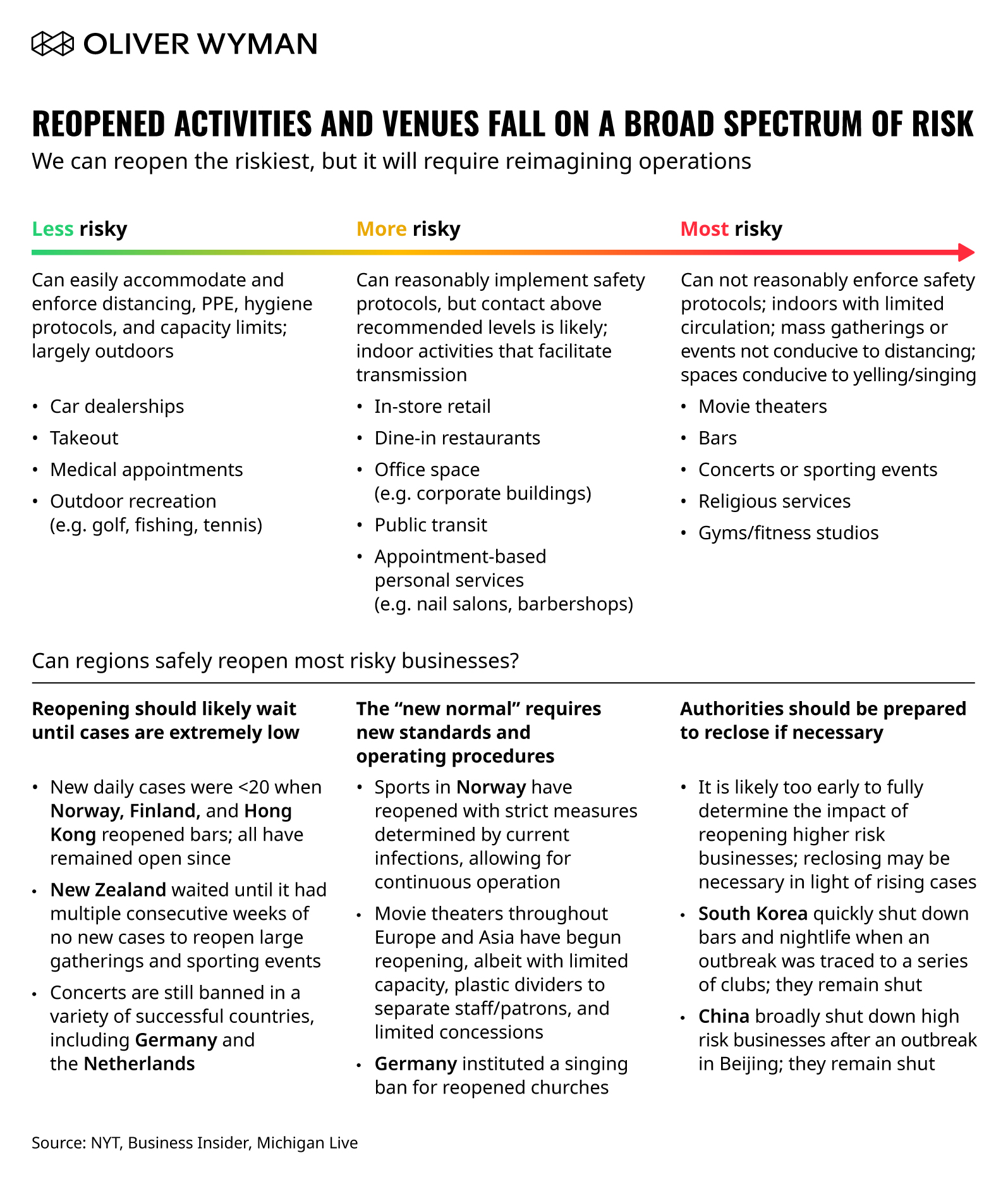
The past six months have helped clarify which activities and venues pose the greatest risks and which ones are relatively safer. We have also learned there is tremendous heterogeneity in transmission – many interactions lead to no transmission at all, while others turn into “super spreading” events. Shifting as much activity outdoors as is feasible is a clear first step, but what about the highest risk settings – bars, restaurants, gyms, and churches? Can we re-imagine operations sufficiently through spacing, reduced capacity, physical barriers, and improved ventilation, or are some of these simply too risky to be opened?
As per the below exhibit, evidence from reopened countries suggests the answer may be yes, but only after active caseload has diminished significantly and with a strong revision of current operations:
4. Learn to use the entire toolkit wisely so we don’t have to use the hammer.
Blunt shutdowns are a crude tool and damage the economy the most. We must learn to purposefully use tools with demonstrated effectiveness.
As we’ve written elsewhere, extensive testing is a smart containment measure that will allow us to detect emerging risks early and deploy targeted suppression measures. Nationally and globally, the impact of COVID-19 is heterogeneous with some communities much more heavily impacted and others relatively untouched. Testing should be conducted both for people with symptoms, as well as random tests of high-risk groups and the general population. Optimal testing levels are indicated by a positive rate of < five percent.
Extensive testing allows for early detection at the local level – it’s critical to pounce on an outbreak early before it precipitates broader lockdowns. Our proprietary Pandemic Navigator suite of forecasting assets allows you to see for a given geography where active cases and thereby hospitalizations are trending over the next several weeks, and helps hospitals and local officials predict when that hospital system capacity will be breached. This is typically a limit when local officials have had to ask businesses to close and citizens to stay home.
But testing alone is insufficient. Public health officials will need to immediately follow-up on positive or suspected cases (infected, or exposed people) to quarantine. Rapid tracing to test close contacts is essential for containing micro-regional outbreaks.
In worksites and other public areas (such as restaurants and retail stores), screen employees for COVID-19 symptoms and require masks for both employees and customers, particularly when people cannot maintain six feet of social distancing. Prohibit those who fail to comply from entering.
5. Aim for broader immunity.
If protective immunity is conferred by infection and lasts at least a year, and vaccine availability in mass scale is not expected for more than a year, we can then consider whether we are comfortable with the risks and implications of purposefully pursuing broader herd immunity through natural infection ahead of vaccine availability.
Let’s assume for the moment that natural infection confers immunity for a year or more. In this scenario, an increase in the total number of cases acts as a brake on the spread of the disease, slowing down the average R(t) of the population proportionally for the same set of activities. For example, if 30 percent of the population is immune by a target date, then R(t) is reduced by 30 percent. This is important because it then means that we can deploy fewer suppression measures to keep R(t) below 1. The benefit of broader immunity is especially important to address seasonality concerns and prepare for a potential large outbreak in the winter.
There may be another brake to slow the spread of the virus in the future. Recent studies have revealed the novel coronavirus is transmitted heterogeneously, meaning some infected people cause very few new infections, while other infected people cause many. This is due to biological and behavioral variations in different segments of the population (for example, 20- to 30-year-olds tend to come into contact with more people than 70- to 80-year olds do). This in turn suggests the threshold for herd immunity may in fact be lower than the figures calculated from homogeneous models. In a homogenous model with R=2.4, herd immunity level is 88 percent, and the herd immunity threshold is 58 percent. We have modeled these variations in biology and behavior as differences in exposure and susceptibility among different segments of the population. Our modeling of this heterogeneous transmission rate suggests a lower herd immunity level on average for the total population, potentially by 20 percentage points or more. This dynamic is a critical input into developing long-term strategies to shield the elderly and other vulnerable populations, and in reducing the herd immunity level required for these sub-populations (for example, targeting <15 percent by the time herd immunity level is achieved) while maximizing herd immunity level for healthy young adults (for example, targeting >90 percent).
The obvious flipsides to these potential benefits are accelerated infections, hospitalizations, and likely even deaths.
What Might the Next Six Months Look Like?
Much of it depends on us. Can we shift our culture and embed critical behaviors into our daily lives across states, employers, and individuals? Can we creatively reopen some of the riskier settings (such as closing streets to traffic to allow for greater outdoor space for restaurants and bars and then shifting to a ski lodge mentality and having people dine outdoors in winter)? Can we protect our elderly and high-risk individuals as the healthier population circulates in society? Can we use data and technology to purposefully direct testing and any required re-closures? Can we accurately predict changes (especially increases) in disease transmission rates? Will the government implement control measures if transmission rates increase alarmingly? Will individuals comply with those measures and adopt changes to their daily routines?
If the answers to these questions are yes, then the second half of the year can begin the process of economic recovery and a return to a re-envisioned normal. Lessons from around the globe make it clear that while eradication is not possible at this moment, a return to public life is.