Preventing Antibiotic Apocalypse By Doing Less, Not More

A staggering one-third of antibiotic prescriptions – nearly 50 million, according to the Centers for Disease Control and Prevention – were unnecessarily prescribed in 2016. This overuse of antibiotics is driving the escalating crisis of antibiotic-resistant bacteria. Each year in the US, “super bugs” such as Methicillin-resistant Staphylococcus aureus (MRSA) infect more than 2,000,000 people, cause 23,000 deaths, and add $20 billion in healthcare costs. Without improved antibiotic stewardship, the societal consequences of antibiotic resistance will skyrocket, leading to what has been called the “antibiotic apocalypse”. By 2050, nearly 320,000 deaths each year in the US could be attributable to antibiotic-resistant bacteria.
There is a simple solution to avoid this prognosis: prescribe fewer unnecessary antibiotics. Defining what constitutes “unnecessary,” however, is surprisingly difficult.
Why It’s Difficult to Prescribe Antibiotics Only when Necessary
Clinical guidelines rarely dictate best practice in absolutes. As a result, there can be a wide divergence in how physicians interpret those guidelines and how they apply them to specific cases. Physicians can rationalize their treatment decisions with little context into whether they are delivering care only when necessary.
Visibility into how individual physician prescription rates for patients with specific clinical presentations vary across peer physicians is a powerful tool in combating overuse. Showing physicians how their practice compares to the practices of their peers – and in the context of established Appropriate Use Criteria – helps physicians define the bounds of appropriate use and self-correct their practices.
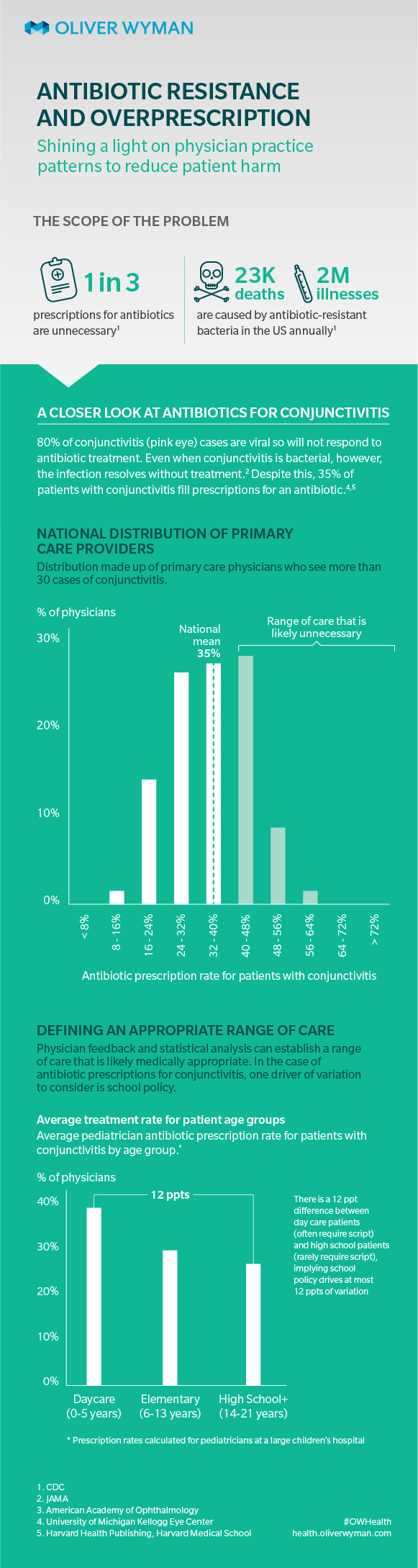
The use of antibiotics to treat conjunctivitis presents a helpful case study. The mean rate and variation in rates at which pediatricians prescribe antibiotics to their patients can be measured through claims data. In a national dataset, physicians had an average of 63 percent of their pediatric patients with conjunctivitis fill antibiotic prescriptions. This is remarkable given that only 20 percent of conjunctivitis cases are bacterial and most of those bacterial cases, if left untreated, resolve on their own in several weeks.
How often should physicians prescribe antibiotics for patients with conjunctivitis? There is no single answer. However, a range of rates indicative of appropriate use can be established by accounting for the drivers of variation. For example, while the overall prevalence of bacterial conjunctivitis is 20 percent, an individual physician’s patient panel may have a higher prevalence (although it should be noted a bacterial case is not automatic justification for an antibiotic prescription). Physicians also cite the “daycare effect” – daycares often require children be on antibiotics for 24 hours before returning to the classroom. Accounting for these and other underlying drivers of variation through a combination of statistical analysis and physician feedback established that any prescription rate (the percent of a physician’s conjunctivitis patients who fill an antibiotic prescription) above 40 percent is unlikely to be medically justified. Yet, 90 percent of physicians prescribe above this rate.
Driving Industry-Wide Change
Physicians can use peer comparison to support conversations among themselves about the appropriate use of antibiotics for conjunctivitis. Remarkable insights emerge from these simple conversations. For example, physicians say there is a significant difference between writing a prescription and asking the patient only to get it filled if necessary, versus asking the patient to fill the prescription and only take the medication if necessary. The bottom line is a patient is more likely to take medication already in his or her hand.
An example of how peer comparison can encourage physicians to reduce inappropriate antibiotic prescribing was highlighted in a recent study where physicians received emails comparing their antibiotic prescribing rates for patients with Acute Respiratory Tract Infections with those who had the lowest prescribing rates in their practice. Eighteen months later, the group which had its individual rates compared to peer rates and received general prescribing guidance reduced its inappropriate prescribing rate by 82 percent. The control group, which only received general prescribing guidance, saw a reduction of only 45 percent.
Transparency into peer practice can help drive a meaningful reduction in the overuse of care.